David Allen Nutrition
Home
About
Team
Shop
Protein Powders
Supplements
Cleanses
Super Foods
Contact
Home
About
Services
Schedule Appointment
Shop
Protein Powders
Supplements
Cleanses
Super Foods
Contact Us
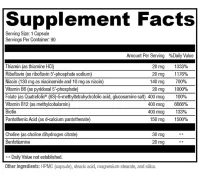
B-Power
$38.76
Quantity
Add to Cart